Quick Facts
Location: Abdominal and pelvic cavity.
Arterial Supply: Ureteric branches of the renal, gonadal, abdominal aorta, common iliac, internal iliac, inferior vesicle, and uterine arteries (females).
Venous Drainage: Same pattern as arterial supply.
Innervation: Through ureteric plexus; Sympathetic: lesser and least thoracic splanchnic nerves, renal, aortic, superior hypogastric, and inferior hypogastric plexuses; Parasympathetic: vagus and pelvic splanchnic; Sensory afferent.
Lymphatic Drainage: Left and right lumbar lymph nodes.




Related parts of the anatomy
Structure/Morphology
The ureters are bilateral muscular tubes that are 25–30 cm long and 0.3 cm wide (Standring, 2016). They extend from the renal pelvis, at the hilum of the kidney, to the ureteric orifices on the internal aspect of the bladder.
The ureters are slightly narrower in three regions: just inferior to the renal pelvis, where it crosses the pelvic brim, and where it enters the urinary bladder. Thus, these are the most likely sites for renal calculi.
The ureters are composed of an inner mucosa lined with urothelium, a submucosal layer, a smooth muscle coat, and an outer adventitial layer.
Anatomical Relations
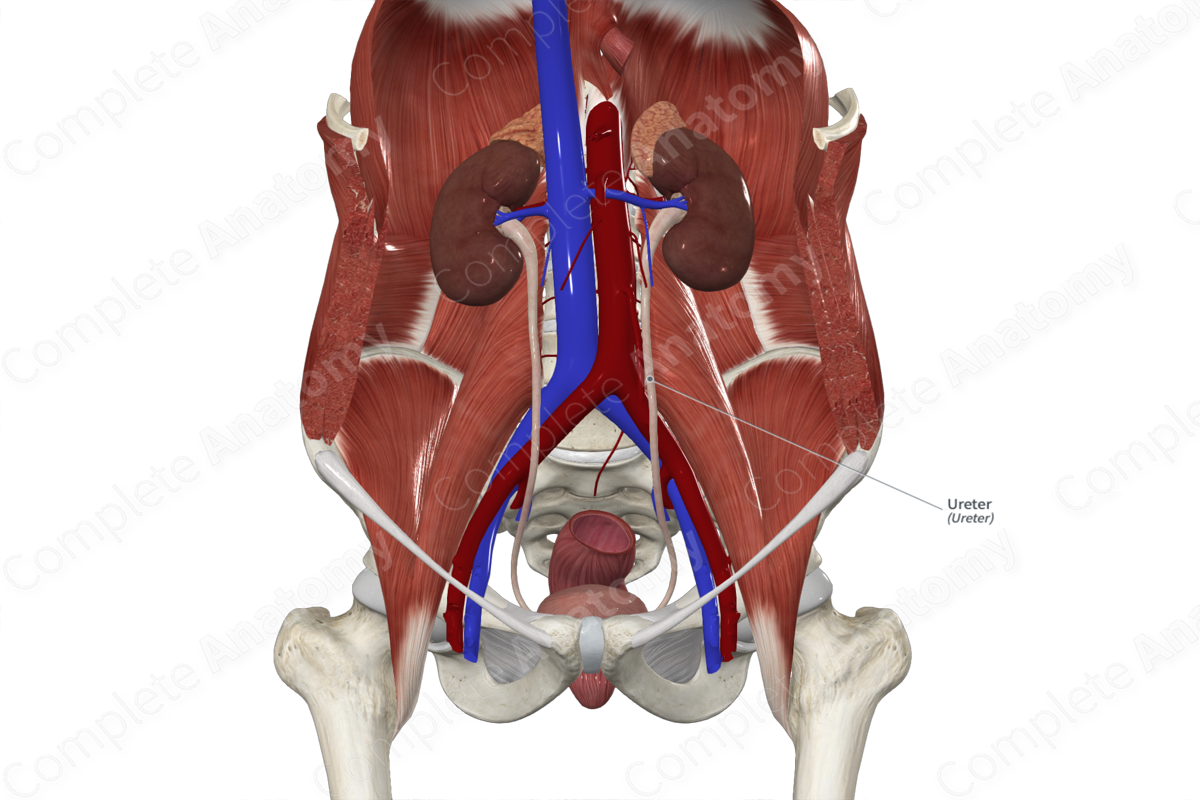
Superiorly, the ureters are a continuation of the renal pelvis as they emerge from the kidneys. They are retroperitoneal and descend within the abdominal cavity. As they travel inferiorly, they sit anterior to the medial edge of the psoas major muscle. This corresponds to the lateral tips of the transverse processes of the lumbar vertebrae. Upon their descent, they pass over the genitofemoral nerves but pass beneath the gonadal vessels.
They cross anterior to the common iliac vessels as they cross the pelvic brim. Firstly, they course in a posterolateral direction and run along the anterior edge of the greater sciatic notch. At the ischial spine, they turn in an anteromedial direction and they approach the bladder.
In males, the ureters pass inferior to the vas deferens and anterior to the superior portion of the seminal vesicle before they then enter the bladder. In females, they sit posterior to the ovary, and then run adjacent to the cervix and lateral fornices of the vagina before entering the bladder.
Finally, the ureters pass through the bladder wall in an oblique manner and end at the ureteric orifices.
Function
The ureters provide a conduit for the passage of urine from the kidney to the bladder. They actively assist in the passage of urine via the peristaltic action of the smooth muscle layer. This is particularly evident in the distal ureter where it has an extra muscular coat. Additionally, the ureters prevent urine reflux due to the oblique passage of the ureters through the bladder wall.
Arterial Supply
The abdominal portion of the ureters is supplied by the ureteric branches of the renal, gonadal, abdominal aorta and common iliac arteries.
The pelvic portion is supplied by branches of the internal iliac and inferior vesicle arteries. In the female the uterine artery also contributes to its vascularization. In the abdomen the branches arise medial to the ureter and in the pelvis, the branches arise on the lateral side of the ureter (Standring, 2016).
There is large variation in the branches that supply the ureters, but longitudinal anastomoses ensure it has adequate vascularization.
Venous Drainage
The ureteric veins that drain the ureters follow the same branching pattern as the arterial supply.
Innervation
Nerves supplying the ureter are located in the ureteric plexus, within the outer adventitial layer, and extend into the muscular layer.
Sympathetic innervation to the ureter arises from the lesser and least thoracic and the splanchnic nerves. The nerves travel to the renal and aortic plexuses (its upper part), from the superior hypogastric plexus and hypogastric nerve (its intermediate part), and from the hypogastric nerve and inferior hypogastric plexus (its lower part) (Standring, 2016).
If present, parasympathetic nerve fibers to superior ureter travel in the vagus nerve, and to the inferior ureter via pelvic splanchnic nerves. The axonal density increases distally, and waves of muscular contraction travel away from the kidney towards the bladder to aid in the passage of urine from the kidneys into the bladder. In addition, nerve endings on the ureteric muscle and on the smooth muscle cells in the walls of blood vessels have been observed and are presumed to be efferent in function (Standring, 2016).
Lymphatic Drainage
Lymph drainage of the superior abdominal portion of the ureter collects in the retrocaval, lateral caval, precaval, and lateral aortic lymph nodes. The inferior portion of the ureter is drained into the common, external, and internal iliac lymph nodes (Földi et al., 2012).
List of Clinical Correlates
—Referred pain
—Renal and ureteric calculi
—Duplex ureters
—Ectopic ureters
—Ureteroceles
—Retrocaval ureters
References
Földi, M., Földi, E., Strößenreuther, R. and Kubik, S. (2012) Földi's Textbook of Lymphology: for Physicians and Lymphedema Therapists. Elsevier Health Sciences.Standring, S. (2016) Gray's Anatomy: The Anatomical Basis of Clinical Practice. Gray's Anatomy Series 41 edn.: Elsevier Limited.
Learn more about this topic from other Elsevier products

Ureter, bladder and urethra histology: Video

Master Ureter, bladder and urethra histology: anatomy, function, and structure. High-yield review with labeled diagrams, videos, and practice quizzes.
