Canadian Cardiovascular Society Issues Updated Guidelines to Assess Private and Commercial Drivers’ Fitness to Drive
April 10, 2024
|
Philadelphia
The Canadian Cardiovascular Society Fitness to Drive Guidelines published in the Canadian Journal of Cardiology provide the latest recommendations regarding driving restrictions for private and commercial drivers who live with cardiovascular conditions
The Canadian Cardiovascular Societyopens in new tab/window (CCS) Fitness to Drive Guidelinesopens in new tab/window have been updated to provide the latest advice on driving restrictions for private and commercial drivers. Using the CCS Risk of Harm formula and available evidence, the Guidelines document the likelihood of sudden cardiac incapacitation and highlight acceptable risk thresholds, providing guidance on when it is and is not safe to allow individuals to resume driving.
Fitness to Drive Guidelines recommendations are aimed at supporting physicians and healthcare providers to advise people with heart conditions about risks and durations for driving restrictions. Updated by a panel of national experts, these new evidence-based guidelines appear in the Canadian Journal of Cardiologyopens in new tab/window, published by Elsevier.
Lead co-chair of the updated Guidelines, Peter G. Guerra, MD, Montréal Heart Institute, University of Montréal, says, "Cardiovascular conditions are among the most frequent causes of impairment to drive, because they might impair circulation of blood to the brain causing mental state alterations via diverse mechanisms like myocardial infarction, cardiac arrhythmias, and heart failure. Accordingly, healthcare providers are often asked to assess fitness to drive in patients with cardiac conditions."
The Fitness to Drive Guidelines build on and update the previous Guidelines that have been trusted and relied upon for two decades. The Guidelines take into account new data on therapies, interventions, and disease entities. These include:
Percutaneous therapies for valvular disease
Genetic disorders
Recent studies looking at the risk of shock or incapacitation in patients with implantable defibrillators
Co-chair Christopher S. Simpson, MD, Queens University, Kingston Health Sciences Centre, explains, "Because there are no randomized trials on Fitness to Drive, observational studies were used to estimate the risk of driving impairment in each situation, and recommendations made on the basis of the CCS Risk of Harm formula, which remains the major, validated assessment tool. More restrictive recommendations were made for commercial drivers, who spend longer average times behind the wheel, use larger vehicles, and might transport a larger number of passengers."
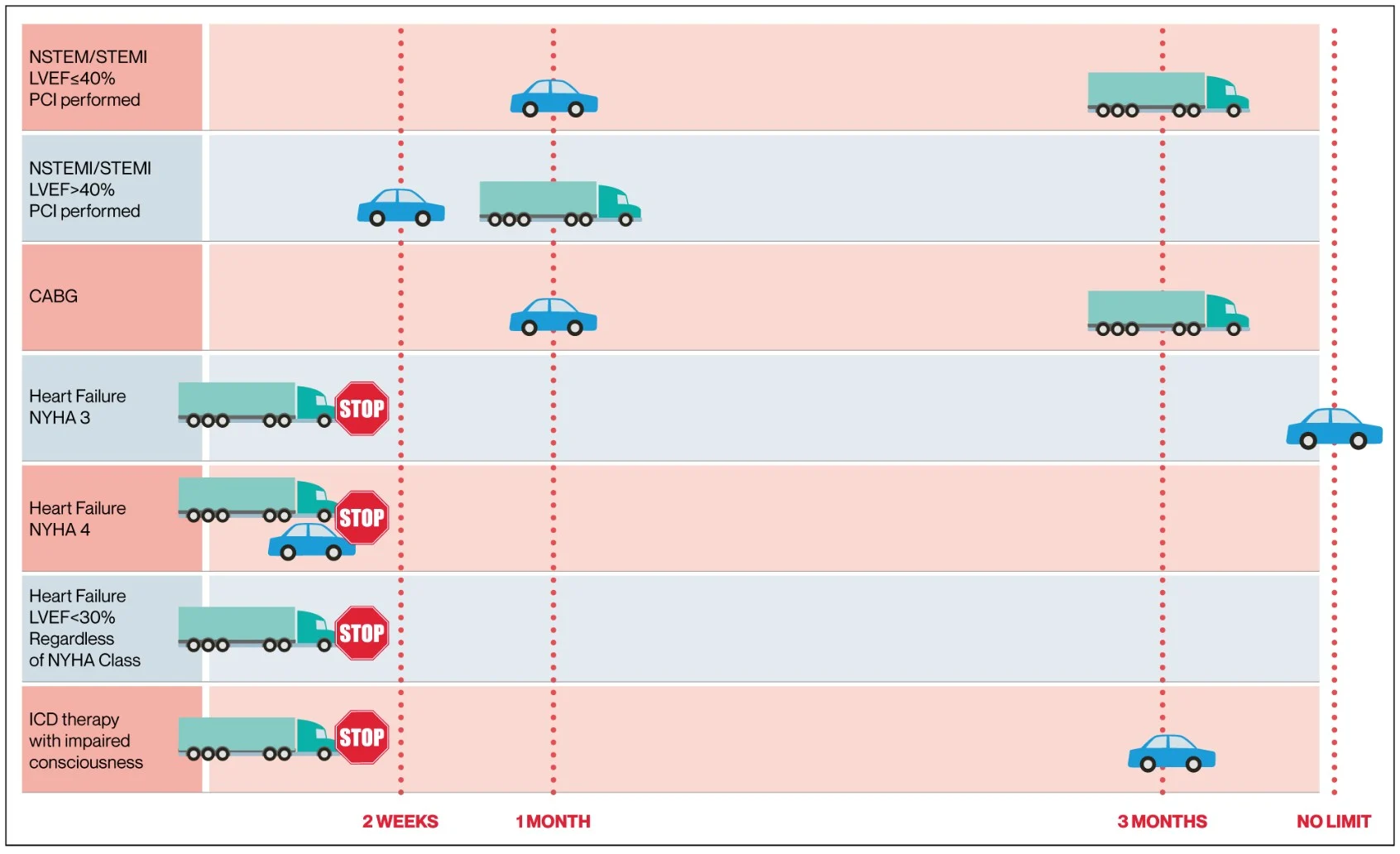
Caption: Fitness to Drive quick reference for common conditions: The car represents private driving, and the truck represents commercial driving (for sake of illustration, this is meant to convey all types of commercial licenses). The timeline on the horizontal axis shows when driving can resume. The “stop” sign signifies complete disqualification. CABG, coronary artery bypass grafting; ICD, implantable cardioverter defibrillator; LVEF, left ventricular ejection fraction; NSTEMI, non-ST-elevation myocardial infarction; NYHA, New York Heart Association; SAVR, surgical aortic valve replacement; STEMI, ST-elevation myocardial infarction (Credit: Canadian Cardiovascular Society).
The Fitness to Drive Guidelines provide recommendations for people with these seven conditions:
Active coronary artery disease
Valvular heart disease
Heart failure, heart transplant, and left ventricular assist devices
Arrhythmia syndromes
Implantable devices (pacemakers and defibrillators)
Syncope (fainting spells)
Congenital heart disease
The co-chairs suggest appropriate waiting times after cardiac interventions or acute illnesses before driving resumption. Short-term driving restriction recommendations were derived, in many instances, based on the risk of harm formula as the evidence used demonstrated diminishing levels of risk over time.
Co-chair Harriette G.C. Van Spall, MD, MPH, McMaster University, Hamilton Health Sciences Centre, and Baim Institute for Clinical Research, Boston, notes, "This document, although not a substitute for clinical judgement or governmental regulations, provides clinicians with a comprehensive list of cardiac conditions and their associated risk of sudden incapacitation. The recommendations can stimulate discussion with patients and inform decision-making regarding private or commercial driving. In some jurisdictions, they will serve as a trigger for clinicians to notify transportation authorities. Adherence to these recommendations can reduce risk to self and others whilst behind the wheel but will not eliminate it."
Dr. Guerra concludes, "If a doctor thinks a driver is a risk, in some Canadian provinces reporting to transportation authorities is mandatory. These are one of the only Guidelines issued for the safety of patients and also for the safety for those around them."
Notes for editors
The article is “Canadian Cardiovascular Society 2023 Guidelines on the Fitness to Drive,” by co-chairs Peter G. Guerra, MD, Christopher S. Simpson, MD, Harriette G.C. Van Spall, MD MPH, Writing Panel: Anita W. Asgar, MD, MSc, Phyllis Billia, PhD, MD, Julia Cadrin-Tourigny, MD, Santabhanu Chakrabarti, MBBS, MD, Christopher C. Cheung, MD, MPH, Annie Dore, MD, Christopher B. Fordyce, MD, MHS, MSc, Pishoy Gouda, MBBCh, Ansar Hassan, MD, Andrew Krahn, MD, Jessica G.Y. Luc, MD, Susanna Mak, MD, PhD, Sean McMurtry, MD, PhD, Colleen Norris, PhD, MSc, RN, Francois Philippon, MD, John Sapp, MD, Robert Sheldon, MD, PhD, Candice Silversides, MD, Christian Steinberg, MD, and David A. Wood, MD (https://doi.org/10.1016/j.cjca.2023.09.033opens in new tab/window). It appears online in the Canadian Journal of Cardiology, volume 40, issue 4, (April 2024) published by Elsevier.
The article is freely available at https://onlinecjc.ca/article/S0828-282X(23)01755-5/fulltextopens in new tab/window.
Full text of the article is also available to credentialed journalists upon request. Contact Astrid Engelen-Visser at +31 6 14395474or [email protected]opens in new tab/window for the PDF or more information. Journalists wishing to speak to the authors should contact Stephanie Naday, Director of Communications/Directrice, Communications, Canadian Cardiovascular Society/Société cardiovasculaire du Canada, at +1 403 828 1017 or [email protected]opens in new tab/window.
About the Canadian Journal of Cardiology
The Canadian Journal of Cardiologyopens in new tab/window is the official journal of the Canadian Cardiovascular Societyopens in new tab/window. It is a vehicle for the international dissemination of new knowledge in cardiology and cardiovascular science, particularly serving as a major venue for the results of Canadian cardiovascular research and Society guidelines. The journal publishes original reports of clinical and basic research relevant to cardiovascular medicine as well as editorials, review articles, case reports, and papers on health outcomes, policy research, ethics, medical history, and political issues affecting practice. www.onlinecjc.caopens in new tab/window
About the Editor-in-Chief
Editor-in-Chief Stanley Nattel, MD, is Paul-David Chair in Cardiovascular Electrophysiology and Professor of Medicine at the University of Montreal and Director of the Electrophysiology Research Program at the Montreal Heart Institute Research Center.
About the Canadian Cardiovascular Society (CCS)
The CCSopens in new tab/window is the national voice for cardiovascular clinicians and scientists, representing more than 2,300 cardiologists, cardiac surgeons and other heart health specialists across Canada. We advance heart health for all by setting standards for excellence in heart health and care, building the knowledge and expertise of the heart team, and influencing policy and advocating for the heart health of all Canadians. For more information about the CCS visit https://www.ccs.caopens in new tab/window.
About Elsevier
Elsevier is a global leader in advanced information and decision support. For over a century, we have been helping advance science and healthcare to advance human progress. We support academic and corporate research communities, doctors, nurses, future healthcare professionals, and educators across 170 countries in their vital work. We help impact makers achieve better outcomes with research and clinical-grade solutions built on the world’s leading evidence-based scientific and medical content, precision AI, and expert human assessment. We champion inclusion and sustainability, working with the communities that we serve. The Elsevier Foundationopens in new tab/window supports research and health partnerships around the world.
Elsevier is part of RELXopens in new tab/window, a global provider of information-based analytics and decision tools for professional and business customers. For more information, visit www.elsevier.com and follow us on social media @elsevierconnect.
Contact
AE